
{kind=link}
One lapse by just one individual can precipitate a domino effect to initiate a cascade of spread of the infection again.
While India has outperformed itself with flawless and precision-implementation of our largest and safest vaccination campaign, there is a road ahead to be traversed. This has been echoed by medical experts globally and by world health bodies too.
This festive season must bring joy and happiness, not disease or despair. Appropriate precautions are the mantra to tide over this last phase of this tempest.
We are at a critical point of our continuing fight against this pandemic. One lapse by just one individual can precipitate a domino effect to initiate a cascade of spread of the infection again. Much can be lost by arrogance or ignorance or indifference. We cannot let that happen now.
Covid-19 is a bushfire-like binary transmission—a spark anywhere is an inferno everywhere.
So let us all, as one team India, buckle up, mask up and vax up.
Let’s address few critical aspects on scientific grounds:
- SOCIAL GATHERING: Crowds, clusters and closed spaces are a recipe for disaster. The SARSCoV2 spreads up to 60 feet in micro aerosol forms and can travel from one room to another, which is called, long jump Covid. A fleeting contact of a mere 15-30 seconds in a room where a potential carrier has been there hours back, is sufficient to cause infection. The Covid causing particles remain suspended for up to 9.2 hours; more so with coughing, shouting, sneezing etc. Even 1% of carriers cause 99% of infections in a cohort. These are called as super spreading events and are thus best avoided. Close proximity within 6-10 feet carries the highest risk. In clusters the attack rate of Delta variant infections is 90.4%, up from an already elevated 80% earlier and can potentially infect more than 50,000 lives in 14 days over 10 layers of recurring transmission.
- SARSCoV2 IS AIRBORNE: For indoor and outdoor transmission, multiple physics studies have shown worldwide that the infection lingers in the air for many hours.
 Much debate has occurred on whether the virus is aerosol borne or droplets borne. It’s both. So it’s abundantly clear that precautions are critical. Indoor transmission is a common mode of reinfection and spread.
Much debate has occurred on whether the virus is aerosol borne or droplets borne. It’s both. So it’s abundantly clear that precautions are critical. Indoor transmission is a common mode of reinfection and spread.
- VENTILATION AT HOME AND OFFICE: Poorly ventilated rooms and shared AC ducts have great potential to spread the virus. This happens even in washroom areas on flushing the toilet, especially with poor exhaust and ventilation mechanisms. Sewage and fecal matter can transmit the virus.
- DELTA VARIANT: The WHO, a few months ago, categorised it as a “variant of concern” and “variant of interest” (VOC and VOI).
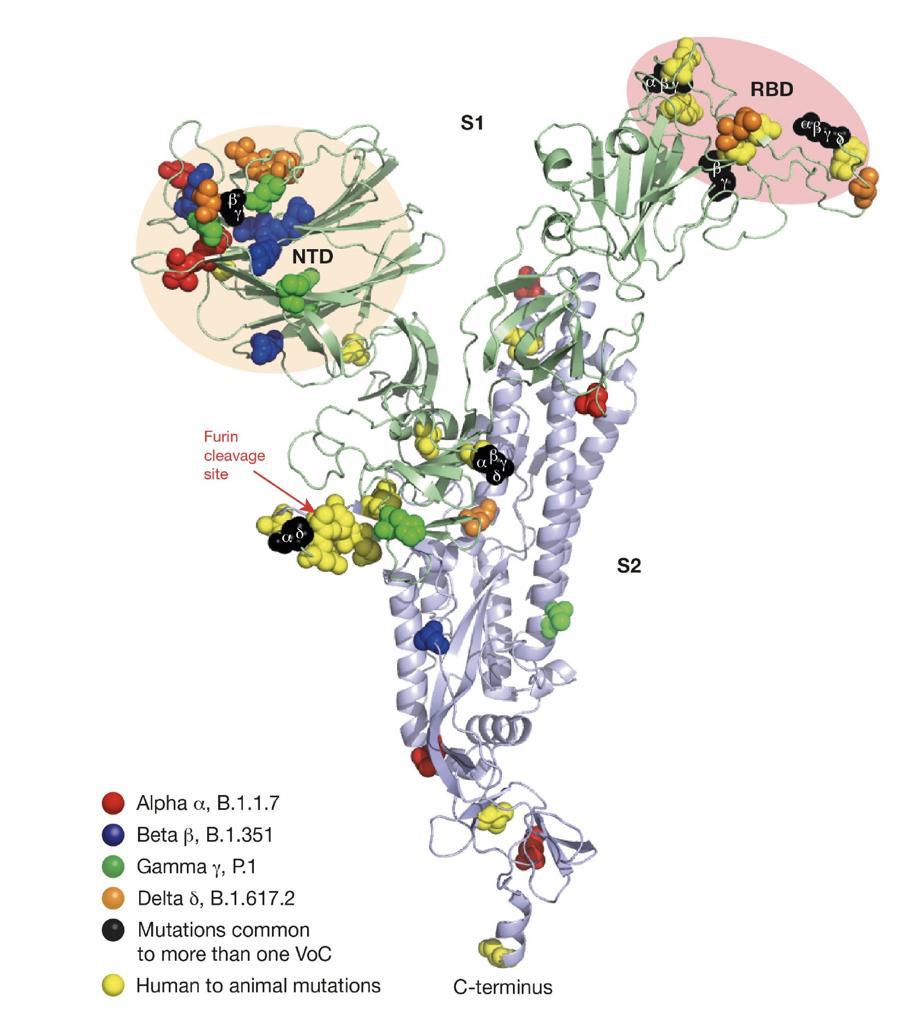
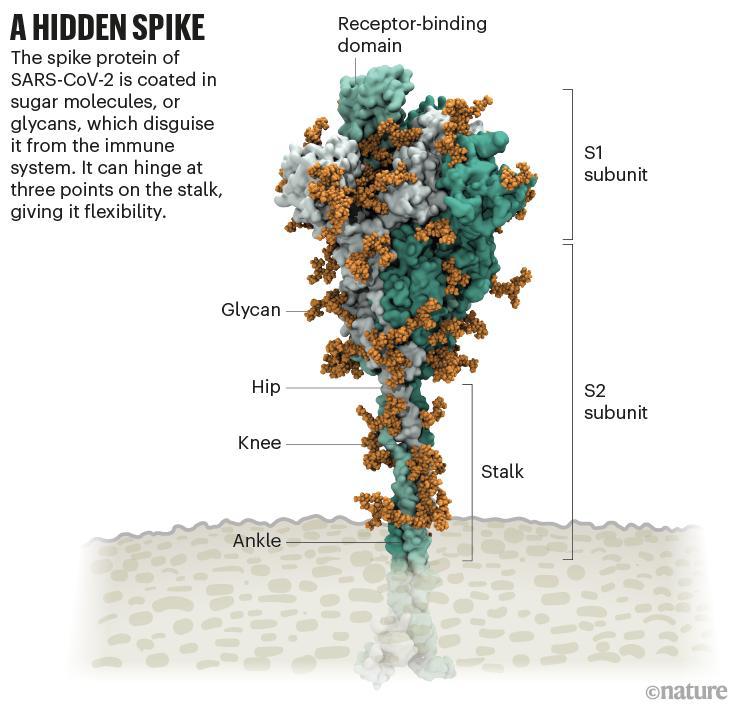
The viral genome has 1,273 base pairs of protein amino acids. RNA viruses always mutate to survive, changing their structure and characteristics and impact. This is viral evolution. The Delta variant contains 38 mutations which make it carry 1,250 times more viral RNA load on Day 1 of the infection, up to 70 times more transmissibility, making it more lethal and infectious. This increases the infection rate by 100 times, hospitalisation in ICU-rate by 287 times, and death rate by 137 times. Simply put, Delta is deadly. The mutations are not limited to RBD—receptors binding domain—but involve the OFR platform and NTD-N Terminal Domain regions, making Delta 6.7 times immune resistant and 8.2 times vaccines resistant. This has caused some amount of decreased vaccine effectiveness on the ground. This is the immuno-escape mechanism this variant possesses. The risk of it latching onto the lung epithelium cells via nasal and oral mucosa is higher, the risk of critical pneumonia and acute respiratory distress syndrome (ARDS) is also more. This carries an R0 of up to 8.0. This is one of the most infectious and contagious and invasive virus infections. Delta high ends the viral load on CT value of RT PCR tests, increases the infectivity days’ duration. The Delta’s focus on NTD rearranges the configuration to form somatic hypermutations and super antigens formations with new hotspots of receptors. Delta is for many months the dominant variant worldwide. When compared to the D614G strain (belonging to the basal B.1 lineage), the spike protein contained 8 mutations, including 4 mutations in NTD (T19R, G142D, Δ156–157 and R158G), 2 in RBD (L452R and T478K), 1 mutation close to the furin-cleavage site (P681R) and 1in the S2 region (D950N). This set of mutations was different from that observed in other members of the B.1.617 lineage and other VOCs. Large syncytia expressing the spike protein were observed in cells that were infected with the Delta variant. The B.1.617 lineage, which is divided into three sublineages according to the PANGO classification, derives from the B.1 lineage (D614G). The 3 sublineages show multiple changes in the spike protein, including the L452R substitution in RBD, which has already been observed in other variants such as B.1.429, and P681R. This substitution is located in the furin-cleavage site and may enhance the fusogenic activity of spike protein. The E484Q substitution—which may be functionally similar to antibody-escape mutation E484K that is found in Beta and Gamma variants (B.1.351 and P.1)—is present in the B.1.617.1 and B.1.617.3 subtypes, and is likely to have reverted in the Delta sublineage, as it was present in a sequence (B.1.617) ancestral to the 3 sublineages. Whether the absence of E484Q, the presence of T478K or other changes in the spike protein or elsewhere may facilitate viral replication and transmissibility remains unknown. Notably, the B.1.617 lineage is not homogeneous, with multiple mutations that are fixed in a sublineage (for example, the spike protein mutations T19R, G142D or D950N) also being detected at lower frequencies in other sublineages.
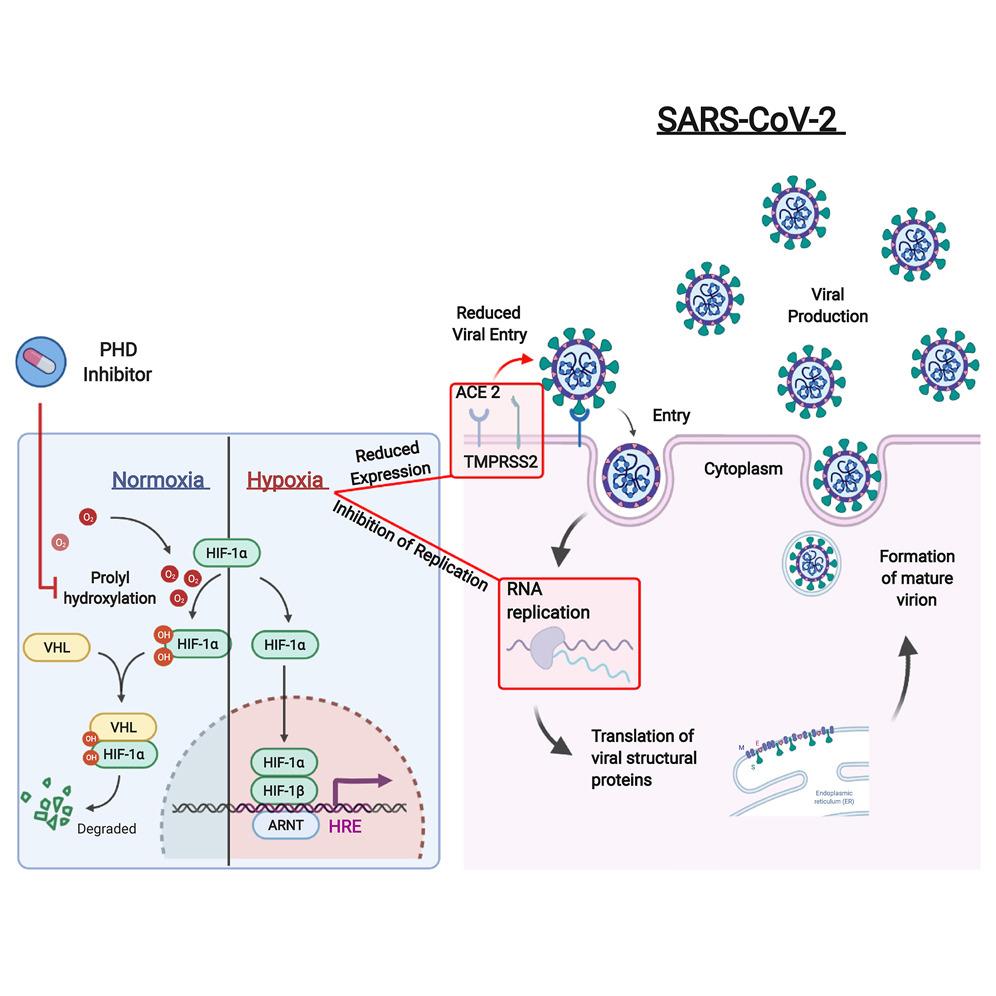 MASKS: Make masks your DNA for the virus, which is an RNA. Masks are easy to wear, easy to use, economical and prevent ingress of transmission and egress of transmission too. The overall mask effectiveness is up to 77% in real world studies. The fine micro particles of sub micron size are stopped up to 35%-45% and coarse particles up to 60%. An N95 mask or a double mask of multi-layered masks is up to 95% protective. Single-layer cloth masks are protective only up to 25%-40%, a bandana face cover 9%, a double layered surgical mask 75%. So the choice is yours. Cover your mouth and nose with well fitted face covering. This isn’t a jewellery item or a fashion statement, to put it above your head or below your chin. The nose must be covered fully, because 80% of the ACE2 Receptor expression is in the nasal passage, and 78% carriers of the virus are in nasal cells post exposure; and the maximum transmission occurs in the first 2 days in the asymptomatic phase, without any clinical signs or symptoms of over 75%-80%. So innocently one can continue to spread this Delta variant without having any symptoms at all.
MASKS: Make masks your DNA for the virus, which is an RNA. Masks are easy to wear, easy to use, economical and prevent ingress of transmission and egress of transmission too. The overall mask effectiveness is up to 77% in real world studies. The fine micro particles of sub micron size are stopped up to 35%-45% and coarse particles up to 60%. An N95 mask or a double mask of multi-layered masks is up to 95% protective. Single-layer cloth masks are protective only up to 25%-40%, a bandana face cover 9%, a double layered surgical mask 75%. So the choice is yours. Cover your mouth and nose with well fitted face covering. This isn’t a jewellery item or a fashion statement, to put it above your head or below your chin. The nose must be covered fully, because 80% of the ACE2 Receptor expression is in the nasal passage, and 78% carriers of the virus are in nasal cells post exposure; and the maximum transmission occurs in the first 2 days in the asymptomatic phase, without any clinical signs or symptoms of over 75%-80%. So innocently one can continue to spread this Delta variant without having any symptoms at all.- VACCINATION: Vaccination saves lives. The global data of CDC of millions of vaccines have proven to decrease the infection rate by 8 times, decrease ICU admissions by 25 times and death rate by 25 times.
Both vaccines being used in India have proven to have more than 90% protection rate with a very low breakthrough infection rate of just 0.2%.
The total of 100 crore vaccines in 275 odd days has been commendable and praiseworthy. The first 10 crores took 85 days, but now the acceleration is excellent even in the remotest areas. The start, like globally, was cautious. Because these were new R&D vaccines, used in a disease which was and is continuously evolving, and because of initial lockdowns and social restrictions. Vaccines will suppress the infection, and post vaccination, one can still be a carrier of the infection, but severe disease and death will be prevented. There have been no significant side effects and reactions. Naysayers have been muted by these vaccines.
- MENTAL HEALTH: The mental health of a nation is important. Covid-19 has exaggerated these hidden symptoms of mental illnesses. Globally, the incidence has increased from 29% to 49% odd. The government and Prime Minister Narendra Modi broke down this long marathon into smaller parts to keep India united in the most troubled times. The occasions to clap or light a lamp are psychological strengths for a country. The biggest battles are won in the mind first.
- LONG COVID-19: More than 50 meta analysis studies have shown that more than 84% symptoms stay at the end of 4-6 weeks post recovery and 54% at 6 months and a few linger until one year on. Fatigue, weakness, cough, cognitive impairment, brain fog, memory issues, cardiac involvement of cardiomyopathy and myocardial inflammation are also seen. Kids-loss of grey and white matter in the brain can have devastating effects for months on end.
- MISINFORMATION AND VACCINES HESITANCY: Every first vaccinee must get the second done at a gap of 12 weeks for Covishield and 4 weeks for Covaxin injections. There is no organ damage. Anyone spreading anti science is doing a disservice to the world.
- WAY FORWARD: A) Paediatric vaccines: These are vital since children are 40% of the Indian population and are the most vulnerable. Kids carry the same viral load as adults, where transmission is equal or more than adults, and can infect parents and elders at home. World data has a vaccine efficiency of 83%. 20% of kids land up with long Covid symptoms. Covaxin should be used soon for 2-18 years with approximately 77-78% efficacy. Schools have been widely recognised as transmission hubs of the infection. So safe reopening of schools mandates us to keep children safety on high priority—the need is for paediatric vaccination, redoing of school ventilation technology, ensure full vaccination of all teachers, etc. Children incidence has doubled up to 22% as per CDC data. Though few get severe disease and MIS-C, but 49.5% of children are asymptomatic carriers and have similar risk of long Covid symptoms.
- B) Pregnancy vaccines: These are vital since pregnancy in unvaccinated ladies increases the complication rate by 50%, also increases the possibilities of still births, premature deliveries, and infant compromised.
- C) Boosters: Boosters have been approved in 40+ countries. The reason is waning immunity post 2 doses of a vaccine. The third dose boosts it up by 8-54 times. Mix and match regimes have been in use in 12 different combinations of Moderna, Pfizer, JJ, AZ. Excellent results so far for prolonged performance, but in India the first aim must be to get double vaccinations in maximum numbers.
- GLOBAL DATA AND PARAMETERS: In spite of all odds, India has 6 times lower the rate of mortality than US or UK.
- AIR POLLUTION, WINTER TEMPERATURE AND ENVIRONMENT: Cold temperatures and environmental factors increase the spread of the virus. Every degree of increase in PM2.5 increases the transmission of SARSCoV2. Hence, Diwali can be a fertile spreading ground. So be cautious.
- Lifestyle diseases (NCD, Non Communicable Diseases) matter more than ever before. We’ve worshiped lifestyle and not life. We have Mirrored: Me-I-Myself and Us or We.
- POST COVID ERA AND LIFE: Mask up for a very long time. Work from home. Digital technology, less physical presence, home care, ambulatory care, telemedicine, preventive care are all core for the future.
- LESSONS FROM SECOND WAVE: The world had never seen such devastation. When we had over 4 lakh new cases per day, with the majority needing hospital care and most being oxygen dependent. All the world quickly learned that there is no country which can cater to such an avalanche of cases. The oxygen crisis emerged and the Indian government swiftly went into military mode to manage this and well they did. Florida, Texas etc in the US are still reeling from this storm. But we can’t repeat the same old mistakes as a society. No government can manage an extremely sick large population. So it’s our collective responsibility. Our commitment to our nation to be responsible citizens.
Let us celebrate Diwali this year with all care, with a prayer for the thousands who lost their lives in this catastrophic pandemic and for the doctors who died on the line of duty. We owe this to our great nation. The next few months will define our next many years. Let’s be a chain of caution and not transmission.
Prof Dr Sanjeev Bagai, Padma Shree, is Chairman, Nephron.